The amount of misinformation surrounding the pandemic is mind-boggling. I feel like I need to research every fact thrown out by the media experts, and even then they seem hard to decipher and verify. It is easy to see why Americans are so distrustful of the information they receive from the government as the message has never been consistent. Below are 7 misconceptions that seem to be thrown around as facts.
1. Social distancing of 6ft is ideal
The CDC says 6ft – the world health organization (WHO) and our schools say 3ft – researchers at MIT say 27 ft. Am I to believe that the laws of physics change as my child walks into school? The reality is no one really knows what social distance is ideal. The origins of the 6ft rule date back to the late 1800’s when a german fella was studying expiratory droplets and noted they travel up to 6ft. Then in the 1930s, William Wells was studying tuberculosis and began to focus on droplet size during cough and sneeze. He found 3ft was likely the number for larger particles which were felt to be the dominant source of infection.
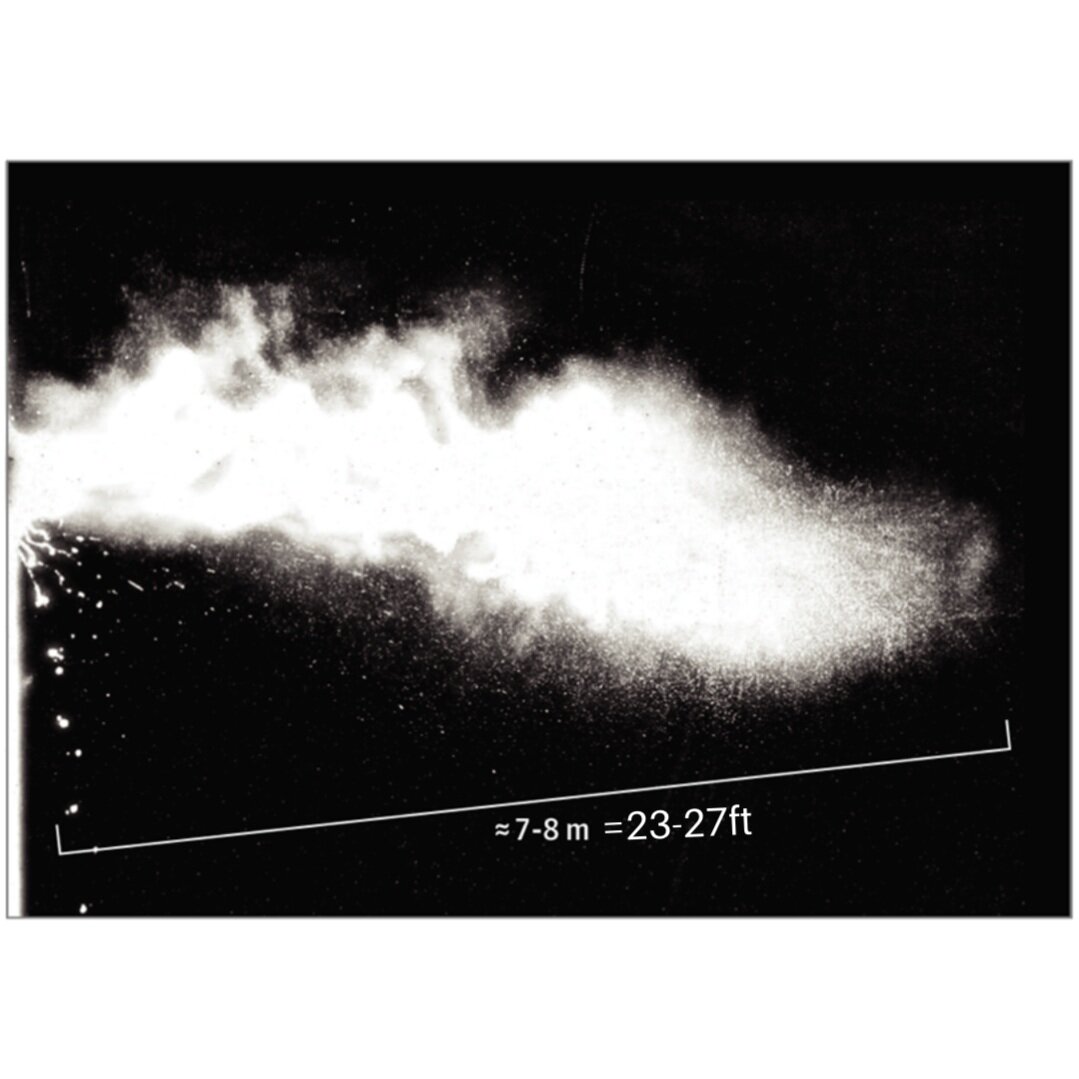
More recently, evidence has mounted that it’s actually the tiny droplets that become aerosolized which are the primary spreader of airborne Covid, particularly in the context of so-called “super-spreader” events. Researchers at MIT recently tested this theory of aerosolized spread and found these droplets quickly spread up to 27 feet. Additionally, they found the temperature and ventilation characteristics of the room played a large role in the spread. The picture below shows a human sneeze quickly spreading to 27 feet.
The reality is that 3 ft versus 6 ft is largely irrelevant from a social distancing standpoint. A focus on ventilation is likely much more important in reducing spread.
2. The use of facemasks dramatically reduce transmission of Covid-19
In my home state of North Carolina we have had a yoyo policy on wearing masks – mask on, mask off, mask on – mask if you want, masks on Wednesdays, masks while you walk the 10 feet to your restaurant table, etc. So do masks really make a difference? First, we need to differentiate a mask from a respirator.
A surgical mask is a loose-fitting, disposable device that creates a physical barrier between the mouth and nose of the wearer and potential contaminants in the immediate environment. These are often referred to as face masks, although not all face masks are regulated as surgical masks. Note that the edges of the mask are not designed to form a seal around the nose and mouth.
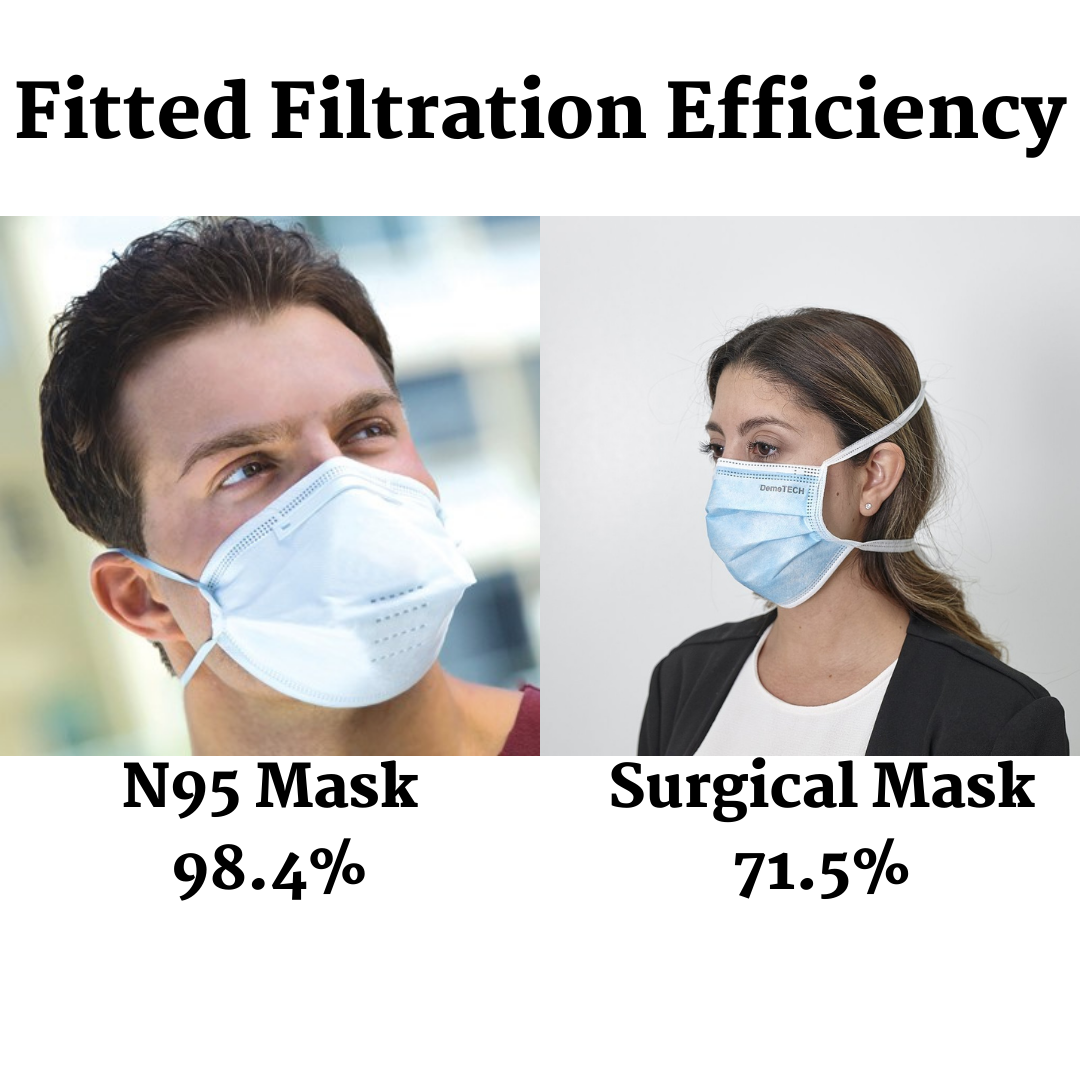
An N95 respirator is a respiratory protective device designed to achieve a very close facial fit and very efficient filtration of airborne particles. Note that the edges of the respirator are designed to form a seal around the nose and mouth. Surgical N95 Respirators are commonly used in healthcare settings and are a subset of N95 Filtering Facepiece Respirators (FFRs), often referred to as N95s.
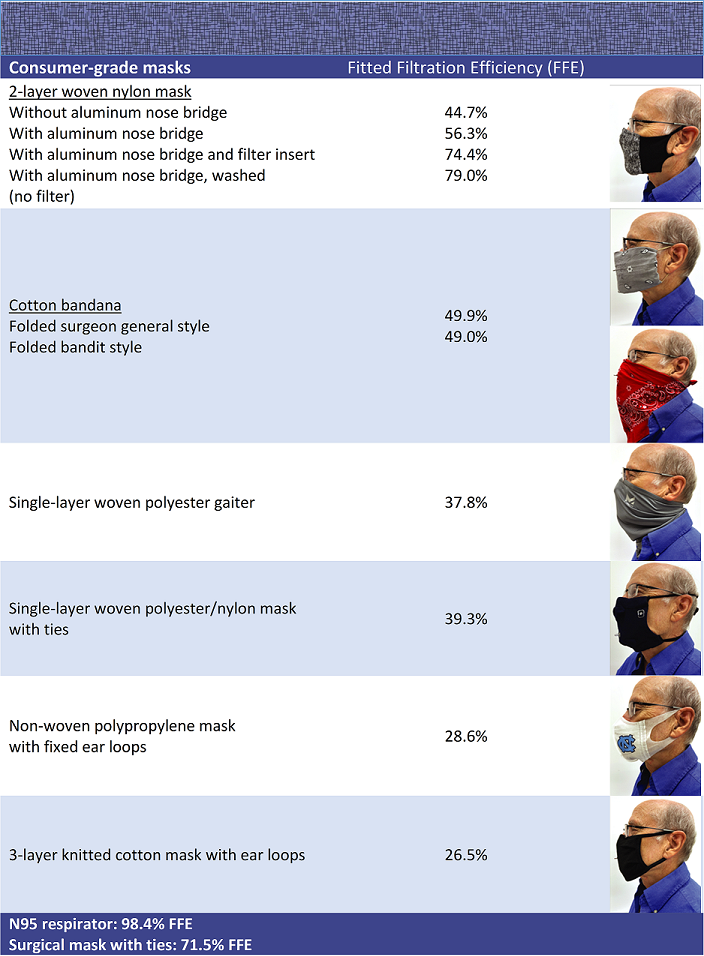
The Environmental Protection Agency (EPA) studied how effective these masks are in addition to many other masks variations you see in the local grocery store. The results vary dramatically as seen below.
A number of studies and meta-analyses have been performed to answer how effective these masks are. Early studies were all based on previous infectious outbreaks of Flu and SARS. The results of the randomized controlled studies were incredibly mixed were in favor of wearing face masks vs. no masks, but not at statistically significant levels. An RCT out of Denmark in 2020 similarly showed no significant reduction in Covid rates with mask use, but a trend toward protection. There is really no evidence masks are beneficial outside other than a few case reports and a discredited study.
The CDC lists an abundance of evidence on their website for mask use. It is important to note almost all of the evidence there utilizes infection rates before and after mask mandates. Thus, they looked at Covid rates in states or cities before and after mask mandates. Many of these studies show a reduction in infection rates after the mask mandates. The problem with these studies is they don’t consider confounders – which are other variables that may be actually causing the decrease in infection rates.
For example, when a city sees a rise in cases and the mayor enacts a mask mandate, does the behavior of its inhabitants change dramatically – going out less, increased social distancing, avoidance of mass gatherings – and these are responsible for the lower infection rates rather than the masks. It’s like saying the oceans have been getting warmer since the number of pirates has decreased – you are attributing the warming to the wrong thing!
The bottom line – masks probably have some mild effect on reducing infection rates, though NOT dramatic. It is reasonable for people at high risk to wear a mask.
3. Vaccination immunity is better than natural immunity
I have written about this in my previous blog on the vaccine and children. Our immune systems are incredibly complex systems that we don’t completely understand – but I do understand the arrogance to believe that our man-made vaccine works better than hundreds of thousands of years of evolution. Our current vaccines give antibodies to one part of the virus, the spike protein. But a virus is made up of more than just a spike protein!
“To date, most studies of natural antibodies that block SARS-CoV-2 have zeroed in on those that target a specific portion of the spike protein known as the receptor-binding domain (RBD)” says Dr. Francis Collins from the NIH. The NIH published a study that showed 84% of antibodies made by people infected with COVID-19 are targeting other parts of the spike protein. Not to mention that there are many other immune system cells involved in defending our bodies against COVID-19. One such group of cells, the T-cells, don’t attack the virus, but rather destroy infected cells. These cells appear to work regardless of COVID strain mutations and may provide longer-term protection – NIH. However, only a few specialized laboratories offer this test. Lastly, even if you have a “good” number of cells, we don’t know what that means clinically.
In summary: We do not have enough reliable or accurate data to indicate how long the immune system is active against COVID-19 after infection or after immunizations. This viral strain is very new! The data is murky! People are scared!
The bottom line – read my other in-depth post on COVID vaccine and Kids.
4. Children tend to be super-spreaders of Covid-19
For a number of common childhood ailments, children are known to be primary vectors of disease – from colds to chickenpox, to RSV, to gastroenteritis – but Covid is NOT one we can blame on them. Listen, I love to blame my kids for everything – stealing my clothes, losing my keys, and taking my husband’s fingernail clippers (because I can never find the 10 pair he has bought me). But when it comes to Covid, it appears the superior immune system of our kids plays a major role.
Studies out of Korea and Italy have shown that children have very low levels of spread in educational settings. In fact transmission from teacher to teacher or from teacher to student is much higher than student to student. An Australian study of 39 COVID-19 cases among 32 students and seven staff traced contacts across 28 schools and six early childhood centers and found only 33 secondary positive cases (28 students and five staff members) out of 3,439 close child contacts and 385 close staff contacts.
What does concern me is the isolation we have forced upon our children. Rates of child/teen depression, anxiety, and suicide attempts have reached all-time highs during the pandemic. And although children are clearly not the problem in the pandemic, they seem to be taking the brunt of the social implications. These effects will likely play out for years to come.
The bottom line – let’s stop blaming the children for being the main spreaders of COVID
5. The 3 vaccine options in the United States are very similar
The vaccines developed by Pfizer and Moderna are very similar so we will discuss those together. These vaccines use a new technology called mRNA coding. Unlike vaccines that put a weakened or inactivated disease germ into the body, the Pfizer and Moderna mRNA vaccines deliver a tiny piece of genetic code from the Covid virus to host cells in the body, essentially giving those cells instructions, or blueprints, for making copies of spike proteins. Our bodies then mount an immune response to those spike proteins (that ironically it just made itself). The resulting antibodies and memory cells should then give long-term immunity from the virus.
This is a carrier vaccine, which uses a different approach than the mRNA vaccines to instruct human cells to make the Covid spike protein. Scientists engineer a harmless adenovirus (a common virus that, when not inactivated, can cause colds, bronchitis, and other illnesses) as a shell to carry genetic code on the spike proteins to the cells (similar to a Trojan Horse). The shell and the code can’t make you sick, but once the code is inside the cells, the cells produce a spike protein to train the body’s immune system, which creates antibodies and memory cells to protect against an actual Covid infection.
Both the Pfizer-BioNTech and Moderna COVID-19 vaccines contain polyethylene glycol (PEG). PEG is a primary ingredient in laxatives and oral bowel preparations for colonoscopy procedures, an inactive ingredient or excipient in many medications, and is used in a process called “pegylation” to improve the therapeutic activity of some medications (including certain chemotherapeutics). The Johnson and Johnson vaccine contains polysorbate 80 – and some people who react to PEG will also react to polysorbate 80, so care must be taken.
6. Vaccinated people shed the spike protein
Historically, vaccines used live viruses to render immunity – so that once vaccinated, these people would actually “shed” the virus and infect others. This was true of the smallpox vaccine and is true for Rotavirus, Chickenpox, and MMR vaccines. Oral polio which is still used in some countries but not the US has shedding potential as well. A recent study demonstrated that 25% of infected patients show spike protein in their urine. There have not been any case reports with accurate documentation of COIVD transmission via fecal or urine route.
In the Covid-19 vaccines, no live viruses are used. There has not been any medical evidence to show spike protein in the urine or feces of vaccinated individuals.
Let’s break it down a bit further. During an infection, the entire virus is reproduced, but the COVID-19 vaccines only introduce the mRNA related to one viral protein — the spike protein – no other proteins or genes get transferred.
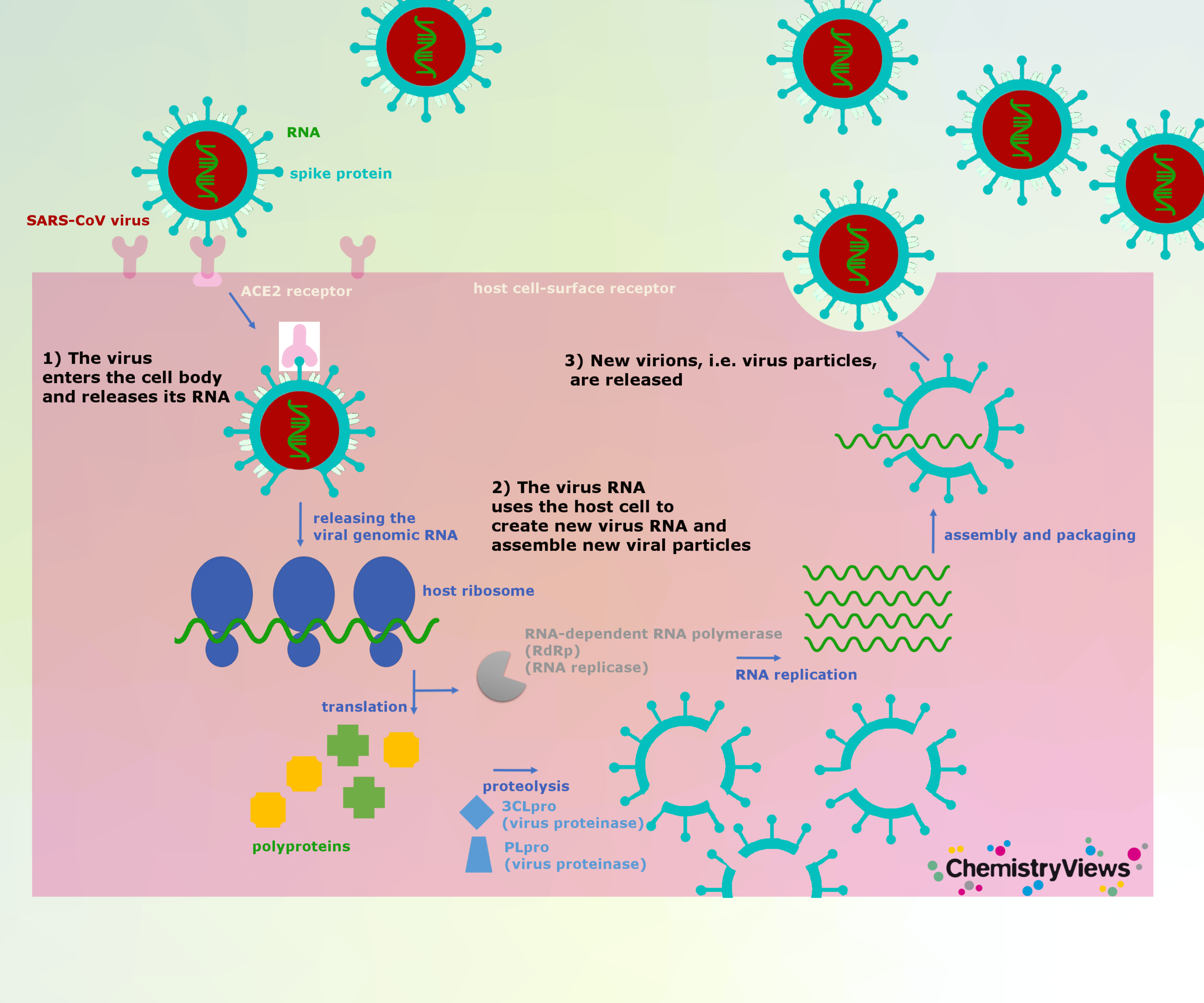
Let’s say, hypothetically, that there are spike proteins from the vaccine shed in the urine and feces; the question on your mind is: Is the spike protein toxic? With an infection, the spike protein attaches to the ACE-2 receptor on our cells which allows for the entire virus to enter and replicate itself (create more viruses). The cell then ruptures and tons of viral particles are released into the body. The more virus particles, the more spike protein, the more inflammation.
Now, hypothetically, let’s say the spike protein from a vaccinated person travels to the unvaccinated person. Hypothetically, the spike protein could attach to the Ace-2 receptor of the unvaccinated person’s cell but it has to evade the immune system: mucous membranes, acids, enzymes, and bodily fluids. The cell would just internalize the spike protein which cannot leave or replicate itself, so no infection occurs. Perhaps a localized reaction can happen, maybe. In studies where the spike protein alone caused inflammation, these proteins were injected into bodies of animals.
What if hypothetically, the vaccinated person sheds mRNA? The vaccines use lipid nanoparticles (fat particles) to surround and protect the mRNA. mRNA on its own is very unstable and very delicate. For a nanoparticle enveloped mRNA to travel out of the body, through the lymphatic system or via circulation and through the liver, intact, and then survive environmental factors has not been demonstrated.
Additionally, another article seemed to suggest that vaccinated persons are shedding spike protein in their urine and feces which is contaminating the water supply and injuring tadpoles. This is far from the truth – the study actually isolated viral toxins from the virus (not vaccinated people) and put them with tadpoles and found neurotoxic effects.
This is an issue that has gotten way out of hand in the media with misinformation. At one point a school in Miami told students not to hug their recently vaccinated parents as they could receive unwanted vaccine shedding. Businesses were posting signs like the one below banning vaccinated persons from entering.
signs like this add to Hysteria!
Lastly, rumors of menstrual issues among women including cramping, prolonged menstruation, or irregular periods. To date no study has ever confirmed this. I treat children 0-22yrs old. To date, none of my teens or young adults have reported this.
Bottom line – there is no evidence that transfer of shedded particles occurs between vaccinated and unvaccinated people. I am keeping an open mind, but the research and biology of viruses and particles do not support this theory. People may be noticing the aforementioned, but I don’t have any medical studies to illustrate what is being observed.
7. If you’ve been vaccinated or had Covid, you can no longer pass the infection to others
Neither the vaccine nor natural immunity from previous infection stops you from becoming reinfected or infecting others during your reinfection. The active immune response in both scenarios cuts down on the amount of virus shed, but that viral shedding definitely has the capacity to infect someone else. Exactly how much of a reduction in shedding occurs with vaccination or natural immunity is still unknown.
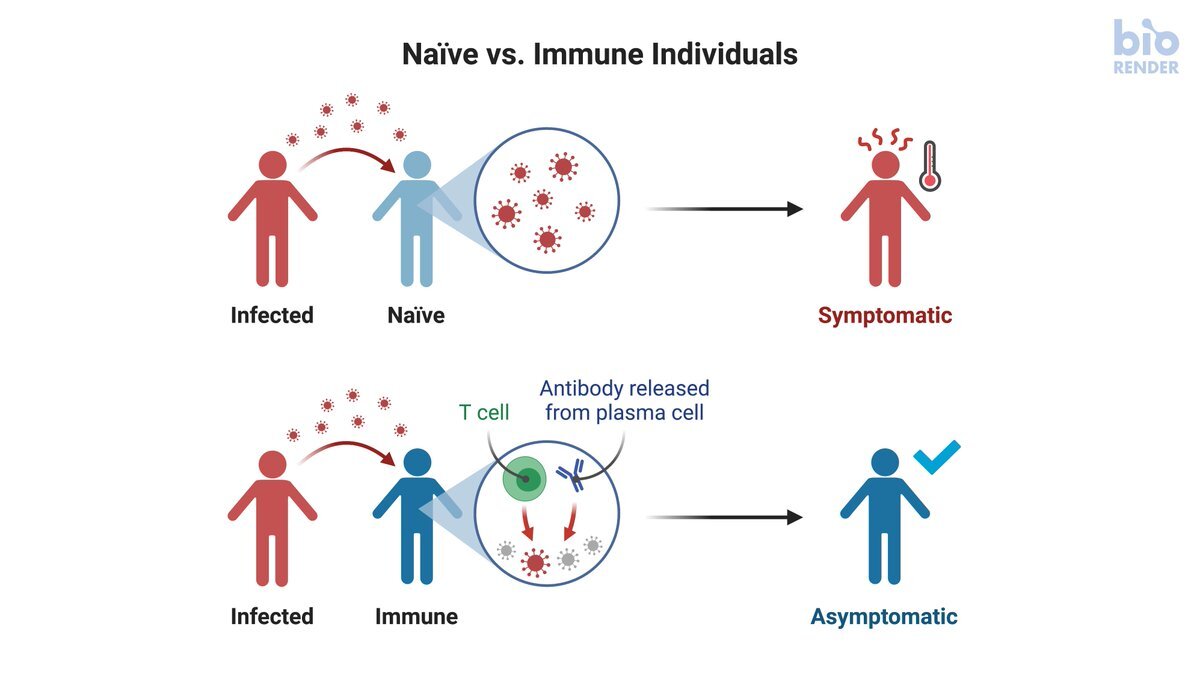
The robust immune response from vaccination or natural immunity also dramatically lessens the severity of the disease, but may also increase the number of cases of asymptomatic infection.
There are hundreds of more myths and misconceptions out there but hopefully, we gave some clarity on a few. One thing that has never been shown to be a myth: a fine-tuned immune system is the number one way to manage the virus. Sign-up for my newsletter or check out my Kick Covid Ass Class to learn ways to power up your family’s immune system.
Yours in Good Health,
Drs. Ana-Maria and John Temple






